State Of Louisiana Medication Order Form
Louisiana Documents Online
State Of Louisiana Medication Order Form
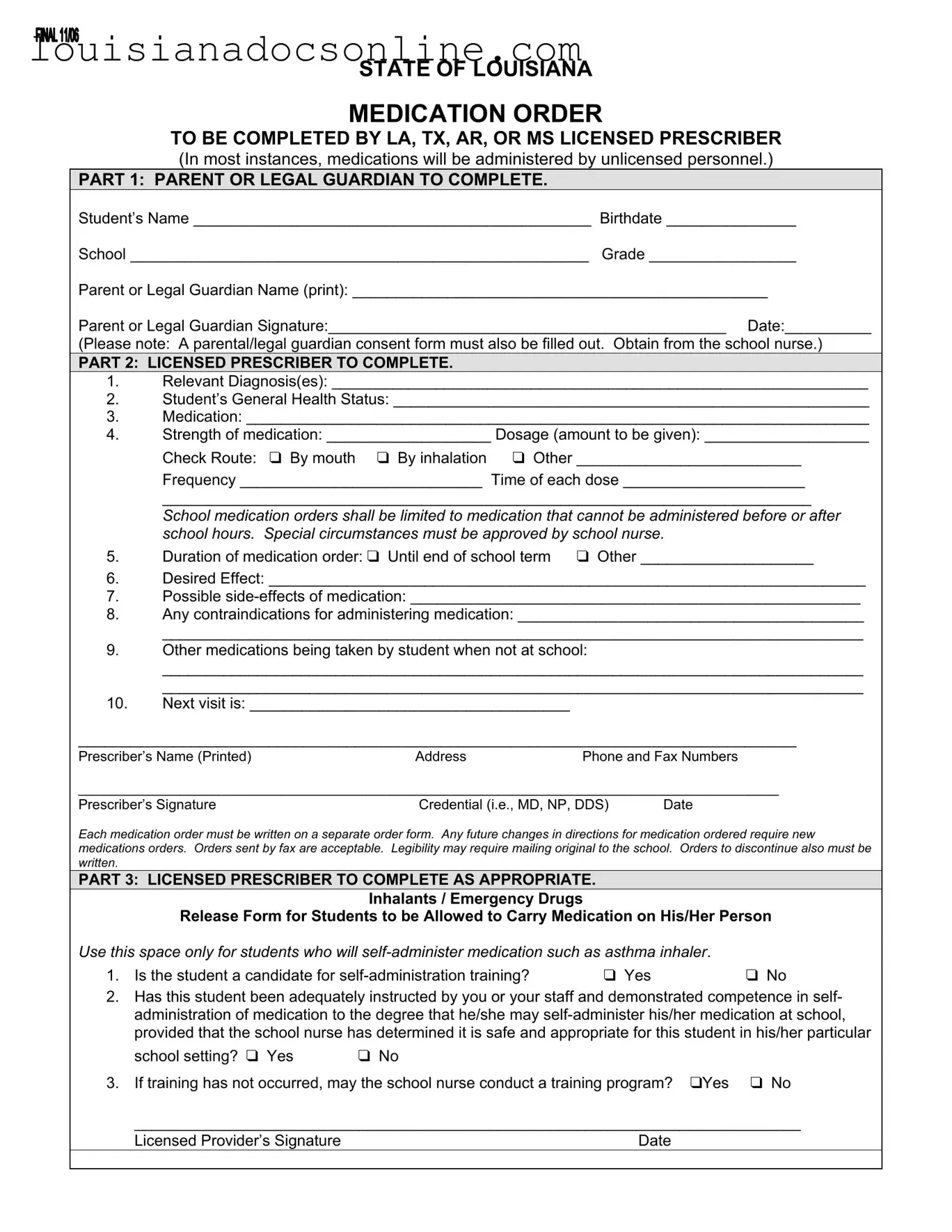
The State of Louisiana Medication Order form is a crucial document designed to ensure the safe administration of medication to students during school hours. This form requires completion by licensed prescribers from Louisiana, Texas, Arkansas, or Mississippi, and is structured in three distinct parts to streamline the process. The first section mandates that a parent or legal guardian provides essential details about the student, including their name, birthdate, school, and grade, alongside a signature to authorize the medication order. The second part is dedicated to the licensed prescriber, who must outline the relevant diagnosis, the student's general health status, and specific medication details, including dosage, administration route, and frequency. Importantly, this section also emphasizes that medications should be limited to those that cannot be given before or after school hours, with special circumstances requiring school nurse approval. The prescriber must also note any potential side effects, contraindications, and other medications the student may be taking. Lastly, the third part addresses self-administration of medications, particularly for students with conditions like asthma, allowing for a tailored approach to individual needs. This comprehensive structure not only facilitates clear communication among caregivers, prescribers, and school personnel but also prioritizes student safety and well-being in the educational environment.
STATE OF LOUISIANA
MEDICATION ORDER
TO BE COMPLETED BY LA, TX, AR, OR MS LICENSED PRESCRIBER
(In most instances, medications will be administered by unlicensed personnel.)
PART 1: PARENT OR LEGAL GUARDIAN TO COMPLETE.
Student’s Name ______________________________________________ Birthdate _______________
School _____________________________________________________ Grade _________________
Parent or Legal Guardian Name (print): ________________________________________________
Parent or Legal Guardian Signature:______________________________________________ Date:__________
(Please note: A parental/legal guardian consent form must also be filled out. Obtain from the school nurse.)
PART 2: LICENSED PRESCRIBER TO COMPLETE.
1.Relevant Diagnosis(es): ______________________________________________________________
2.Student’s General Health Status: _______________________________________________________
3.Medication: ________________________________________________________________________
4.Strength of medication: ___________________ Dosage (amount to be given): ___________________
|
Check Route: ❑ By mouth ❑ By inhalation ❑ Other __________________________ |
|
|
Frequency ____________________________ Time of each dose _____________________ |
|
|
___________________________________________________________________________ |
|
|
School medication orders shall be limited to medication that cannot be administered before or after |
|
|
school hours. Special circumstances must be approved by school nurse. |
|
5. |
Duration of medication order: ❑ Until end of school term |
❑ Other ____________________ |
6.Desired Effect: _____________________________________________________________________
7.Possible
8.Any contraindications for administering medication: ________________________________________
_________________________________________________________________________________
9.Other medications being taken by student when not at school:
_________________________________________________________________________________
_________________________________________________________________________________
10.Next visit is: _____________________________________
___________________________________________________________________________________
Prescriber’s Name (Printed)AddressPhone and Fax Numbers
__________________________________________________________________________________________
Prescriber’s Signature |
Credential (i.e., MD, NP, DDS) |
Date |
Each medication order must be written on a separate order form. Any future changes in directions for medication ordered require new medications orders. Orders sent by fax are acceptable. Legibility may require mailing original to the school. Orders to discontinue also must be written.
PART 3: LICENSED PRESCRIBER TO COMPLETE AS APPROPRIATE.
Inhalants / Emergency Drugs
Release Form for Students to be Allowed to Carry Medication on His/Her Person
Use this space only for students who will |
|
|
1. Is the student a candidate for |
❑ Yes |
❑ No |
2.Has this student been adequately instructed by you or your staff and demonstrated competence in self- administration of medication to the degree that he/she may
school setting? ❑ Yes ❑ No
3. If training has not occurred, may the school nurse conduct a training program? ❑Yes ❑ No
_____________________________________________________________________________
Licensed Provider’s Signature |
Date |
Louisiana Application for Military Discount - Your personal information will be treated confidentially by your insurance company.
It is crucial for sellers and buyers in New York to understand the importance of proper documentation during a sale, which is where the New York Bill of Sale comes in handy. This form not only assists in preventing misunderstandings between parties but also acts as a legally binding record of the transaction. For more detailed information and to access a reliable template, you can visit legalpdf.org.
Louisiana Credentialing Application - Specify the type of practice to help categorize your services correctly.
Louisiana Oversize Permits Cost - Completing this form accurately is key to getting the necessary approvals swiftly.
The State of Louisiana Medication Order form is an essential document for ensuring that students receive necessary medications during school hours. However, several other forms and documents often accompany this order to facilitate communication and compliance among parents, guardians, and school personnel. Here are five commonly used documents:
These documents work together with the State of Louisiana Medication Order form to create a comprehensive approach to student health management in schools. By ensuring all necessary paperwork is completed, schools can provide safe and effective care for students with medical needs.
When filling out and utilizing the State of Louisiana Medication Order form, it is crucial to adhere to specific guidelines to ensure the process runs smoothly and effectively. Here are some key takeaways to consider:
By following these guidelines, parents, guardians, and prescribers can help ensure that students receive their medications safely and effectively while at school.