Louisiana Medicaid Freedom of Choice List Form
Louisiana Documents Online
Louisiana Medicaid Freedom of Choice List Form
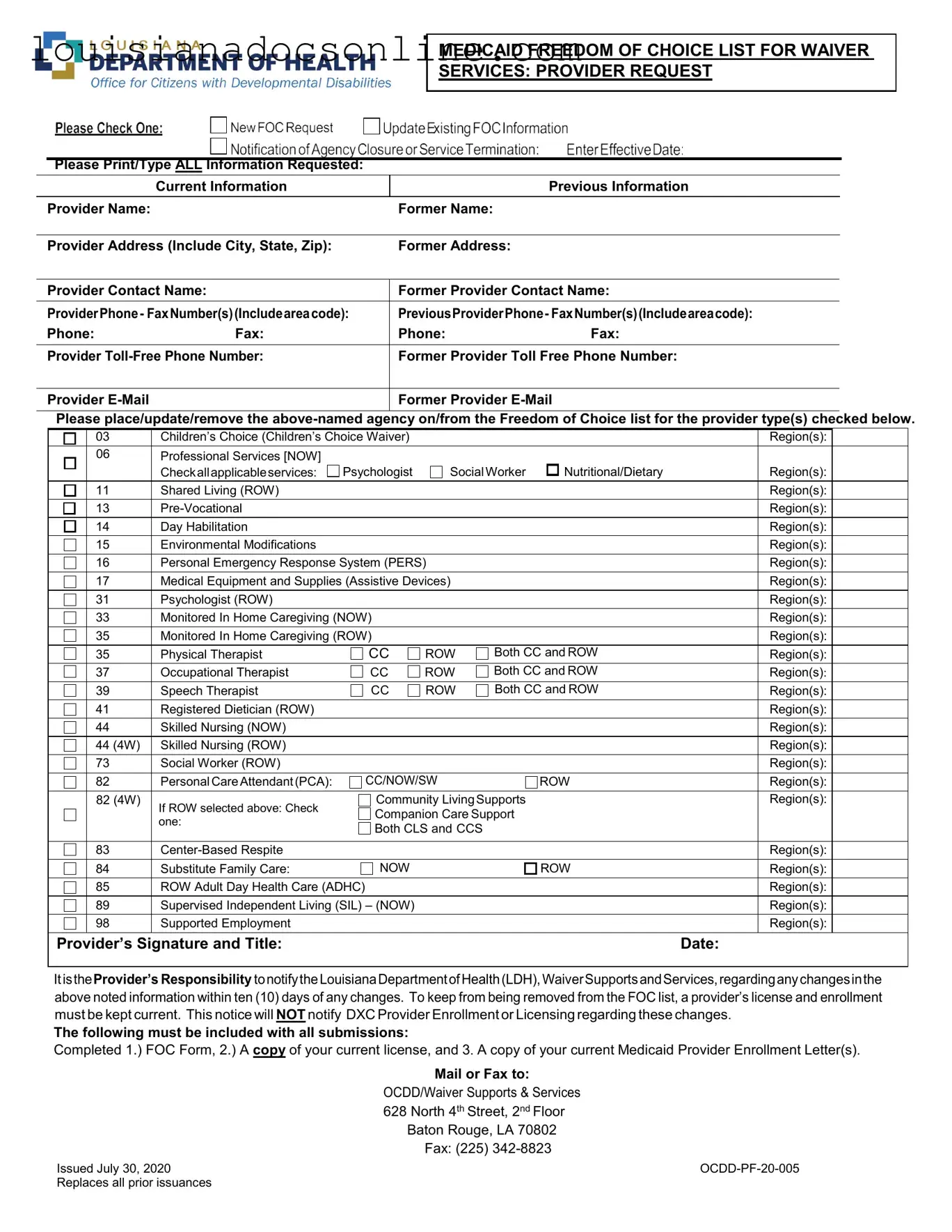
The Louisiana Medicaid Freedom of Choice List form is a critical document for providers seeking to offer waiver services under the state's Medicaid program. This form facilitates the inclusion or removal of providers from the Freedom of Choice list, which is essential for ensuring that individuals receiving Medicaid services can select from a range of qualified providers. It requires detailed information, including the provider's name, address, and contact details, as well as any previous names or addresses. Providers must specify the types of services they offer, which may include children’s choice waivers, personal care assistance, and various therapeutic services, among others. Each service type has designated regions, underscoring the importance of geographical considerations in service delivery. Providers are also reminded of their responsibility to keep their information up to date; failure to do so can result in removal from the list. To ensure compliance, the form must be accompanied by a current license and Medicaid provider enrollment letter, and it must be submitted to the Louisiana Department of Health within a specific timeframe. This process is not just bureaucratic; it directly impacts the quality and accessibility of care for vulnerable populations in Louisiana.
MEDICAID FREEDOM OF CHOICE LIST FOR WAIVER
SERVICES: PROVIDER REQUEST
Please Print/Type ALL Information Requested:
|
Current Information |
|
Previous Information |
|
|
|
|
Provider Name: |
|
Former Name: |
|
|
|
|
|
Provider Address (Include City, State, Zip): |
Former Address: |
|
|
|
|
||
Provider Contact Name: |
Former Provider Contact Name: |
||
|
|
||
ProviderPhone- FaxNumber(s)(Includeareacode): |
PreviousProviderPhone- FaxNumber(s)(Includeareacode): |
||
Phone: |
Fax: |
Phone: |
Fax: |
|
|
||
Provider |
Former Provider Toll Free Phone Number: |
||
|
|
|
|
Provider |
|
Former Provider |
|
|
|
|
|
Please place/update/remove the
|
03 |
Children’s Choice (Children’s Choice Waiver) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
06 |
Professional Services [NOW] |
|
|
|
|
|
|
|
|
|
Checkallapplicableservices: |
Psychologist |
SocialWorker |
Nutritional/Dietary |
|
Region(s): |
|
|
|
11 |
Shared Living (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
Region(s): |
|
|
|
14 |
Day Habilitation |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
15 |
Environmental Modifications |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
||
|
16 |
Personal Emergency Response System (PERS) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
||
|
17 |
Medical Equipment and Supplies (Assistive Devices) |
|
|
|
Region(s): |
|
||
|
|
|
|
|
|
|
|
|
|
|
31 |
Psychologist (ROW) |
|
|
|
|
|
Region(s): |
|
|
33 |
Monitored In Home Caregiving (NOW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Monitored In Home Caregiving (ROW) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
35 |
Physical Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
37 |
Occupational Therapist |
CC |
ROW |
Both CC and ROW |
|
: |
|
|
|
|
|
|
Region(s) |
|
||||
|
39 |
Speech Therapist |
CC |
ROW |
Both CC and ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
41 |
Registered Dietician (ROW) |
|
|
|
|
|
Region(s): |
|
|
44 |
Skilled Nursing (NOW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
44 (4W) |
Skilled Nursing (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
73 |
Social Worker (ROW) |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
82 |
Personal CareAttendant(PCA): |
CC/NOW/SW |
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
||
|
82 (4W) |
If ROW selected above: Check |
Community LivingSupports |
|
|
Region(s): |
|
||
|
|
Companion Care Support |
|
|
|
|
|||
|
|
one: |
|
|
|
|
|||
|
|
Both CLS and CCS |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
83 |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
84 |
Substitute Family Care: |
NOW |
|
|
ROW |
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
85 |
ROW Adult Day Health Care (ADHC) |
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
|
|
89 |
Supervised Independent Living (SIL) – (NOW) |
|
|
|
|
Region(s): |
|
|
|
98 |
Supported Employment |
|
|
|
|
|
Region(s): |
|
|
|
|
|
|
|
|
|
|
|
Provider’s Signature and Title: |
|
|
|
|
Date: |
||||
|
|
|
|
|
|
|
|
|
|
ItistheProvider’s Responsibility tonotifytheLouisianaDepartmentofHealth(LDH),WaiverSupportsandServices,regardinganychangesinthe above noted information within ten (10) days of any changes. To keep from being removed from the FOC list, a provider’s license and enrollment must be kept current. This notice will NOT notify DXC Provider Enrollment or Licensing regarding these changes.
The following must be included with all submissions:
Completed 1.) FOC Form, 2.) A copy of your current license, and 3. A copy of your current Medicaid Provider Enrollment Letter(s).
Mail or Fax to:
OCDD/Waiver Supports & Services
628North 4th Street, 2nd Floor Baton Rouge, LA 70802 Fax: (225)
Issued July 30, 2020 |
|
Replaces all prior issuances |
|
Where to Get T1 - Companies must adequately account for all timber severed or purchased during the reported period.
Before entering into a rental agreement, it's important for both landlords and tenants to familiarize themselves with the stipulations of the lease, including crucial details regarding the rental terms and responsibilities. For those looking for a comprehensive guide, the arizonapdfforms.com/residential-lease-agreement offers valuable resources to ensure clarity and protect the rights of both parties involved in the rental process in Arizona.
Louisiana Up 1 - The form includes details such as holder name and address.
The Louisiana Medicaid Freedom of Choice List form is essential for providers seeking to update their information or request inclusion on the Freedom of Choice list. Alongside this form, several other documents are commonly used to ensure compliance and streamline the process. Below are four key documents that often accompany the Freedom of Choice List form.
By ensuring that these documents are completed and submitted alongside the Freedom of Choice List form, providers can facilitate a smoother process and maintain compliance with Louisiana Medicaid requirements. Keeping all information up to date is essential for continued service eligibility.
When filling out the Louisiana Medicaid Freedom of Choice List form, it is crucial to pay attention to detail. Here are some key takeaways to guide you through the process:
By following these key points, you can ensure a smoother experience when using the Louisiana Medicaid Freedom of Choice List form. Timeliness and accuracy are essential in this process.